 Below is my translation of pages 144-156 of my five-chapter book Hojas Susurrantes. The first chapter has already been translated into English and appears as a separate book, which can be obtained here. As soon as I finish the translation of this second chapter of Hojas Susurrantes, it will also be available as a separate book.
Below is my translation of pages 144-156 of my five-chapter book Hojas Susurrantes. The first chapter has already been translated into English and appears as a separate book, which can be obtained here. As soon as I finish the translation of this second chapter of Hojas Susurrantes, it will also be available as a separate book.
I confess that I still need to proofread once more the translated text below. I will do so after I finish translating the rest of that chapter, entitled “How to Murder Your Child’s Soul”.
I will not be posting another section of my book on this site. The translation below is merely a sample to encourage interested readers to obtain a printed copy once the translation is complete.
______ 卐 ______
Abusive Parents and Psychiatrists:
A Felonious Association
I believe we should ban all psychiatric relationships between adults and children and call child psychiatry by its correct and true name: psychiatric rape.
—Thomas Szasz [1]
Since the terrible events of my adolescence, I had been left with the idea that Dr Amara was simply incompetent in his profession. More than twenty years would pass before I read the critics of psychiatry and psychotherapy. The biggest surprise I encountered when reading these authors was the discovery that, since its inception, psychiatry has sided with parents in conflicts with their children; and it has sided with them regardless of the sanity of the children or the dysfunction of the parents in question.
This means that Amara was not incompetent in his profession. He behaved as psychiatrists have been behaving for a long time.
In the 17th century, the admission regulations for children of families in two French asylums stipulated: ‘Children of artisans and other poor inhabitants of Paris up to the age of twenty-five, who used their parents badly or who refused to work through laziness, or, in the case of girls, who were debauched or in evident danger of being debauched, should be shut up, the boys in the Bicêtre, the girls in the Salpêtrière. This action was to be taken on the complaint of the parents’. [2]
Similarly, in the 18th century, parents could appeal directly to the king to have a rebellious child imprisoned in the Bastille by means of a lettre de cachet.[3] Before the French Revolution, conditions in these asylums were so poor that half of the inmates died each year from malnutrition, cold and disease. Note that both the Bicêtre and the Salpêtrière committed perfectly sane, though rebellious, adolescents for not wanting to work—‘laziness’—or for having premarital relations—‘debauched’. The same stratagem appeared in North America in the 19th century. In 1865, the Boston Times Messenger described the McLean Hospital asylum as a ‘Bastille for the incarceration of some persons obnoxious to their relatives’. [4]
These incredible commitment clauses could be understood if we view psychiatry from a perspective we are not accustomed to: not as it presents itself, an objective science, but as a mercenary profession that, since its origins, has allied itself with the highest bidder. And the highest bidders have not only been parents, but also husbands. In 1851, for example, the admissions regulation in the state of Illinois in the United States stipulated that, ‘Married women… may be entered or detained in the hospital at the request of the husband of the woman… without evidence of insanity required in other cases’. [5]
In our times, psychiatry has become a large pharmaceutical industry that operates within the realities of the market and the laws of supply and demand. The keyword is demand. When family problems arise it is the parents, and only the parents, who have the financial means to pay professionals. Therefore, from their origins, it has been convenient for these professionals to view family problems as medical problems. The cause of this self-deception, as one paediatrician observed, is that ‘teens are Big Business for psychiatrists’. [6]
Between 1980 and 1987, the number of children and adolescents temporarily admitted to American psychiatric hospitals rose by 43 per cent. Social researchers such as Ira Schwartz found that these internments were not due to mental disorders, but rather because the children were at war with their parents.[7] The profession called psychiatry is not geared toward defending these adolescents against their parents. Doing so would put psychiatrists at odds with their natural source of income. In some private psychiatric hospitals in the United States, high-ranking psychiatrists have pocketed between $600,000 and $900,000 annually. Paul Fink, president of the American Psychiatric Association (APA) in the 1980s, stated bluntly: ‘It is the task of APA to protect the earning power of psychiatrists’.[8]
That psychiatrists have played the role of advocates for parents, husbands, and the status quo is seen with extraordinary clarity by studying how doctors diagnosed in the 18th and 19th centuries.
In 1728, Daniel Defoe, the author of Robinson Crusoe, wrote that it was a ‘vile practice’ and a ‘clandestine inquisition’ to ‘send wives to Mad Houses for any whim or displeasure’.[9] Defoe was the first writer I know of who compared psychiatry to the Inquisition. In 1851, when slavery was legal in the United States, Dr Samuel Cartwright discovered that slaves who ran away from their masters suffered from drapetomania (from the Greek word drapetes, which conveys the idea of flight): a mental illness exclusive to blacks who had ‘a delusional desire to flee from their owners’. His discovery was published in the New Orleans Medical and Surgical Journal. Other blacks suffered from dysthesia ethiopica, whose symptom was ‘inattentiveness to private property’. It was believed that a sane Negro was one who behaved docilely toward his master. Benjamin Rush, the father of American psychiatry and one of the signers of the American Declaration of Independence, also discovered several nervous illnesses. He called one of them anarchia and defined it as a brain disease of those dissatisfied with the new American system.[10] Rush invented the Tranquilizing Chair, a device that immobilized his patients for half a day or an entire day. He was also one of the pioneers in conceiving of alcoholism as a biomedical entity. Today, Rush’s portrait still adorns the official logo of the American Psychiatric Association.[11]
In 19th-century Europe, things were no better. As was known since the time of Defoe, men had been using psychiatry to subdue their wives. Those who failed to fulfil the role assigned by society were labelled folie lucide in France (literally ‘lucid madness’) and moral insanity in England and its equivalent in Switzerland and Germany. Many were committed to psychiatric hospitals at the initiative of their husbands, fathers or brothers. In fact, in the 19th century women were the primary target of organized psychiatry, just as children were in the final decades of the 20th century and at the dawn of the 21st.
In 1820, Elizabeth Packard was hospitalized by her husband for freely lecturing on the Bible based on her own reflections. This woman survived her confinement, described what she saw in the asylum and, like Defoe, compared psychiatry to the Inquisition. Jeffrey Masson brought to light other testimonies from women who managed to escape from hospitals and exposed both their relatives and the psychiatrists. Hersilie Rouy, hospitalized at the Salpêtrière due to a dispute with her brother, testified in a book published in 1883: ‘For fourteen years I have lived under an incarceration that cut me off from the real world, took away my civil rights, deprived me of my name, took away everything I owned, destroyed my entire existence without even being able to say why’.[12] It is worth mentioning that the famous physician Jean Martin Charcot, who is credited with researching hysteria in women, was running the Salpêtrière when Hersilie was imprisoned.
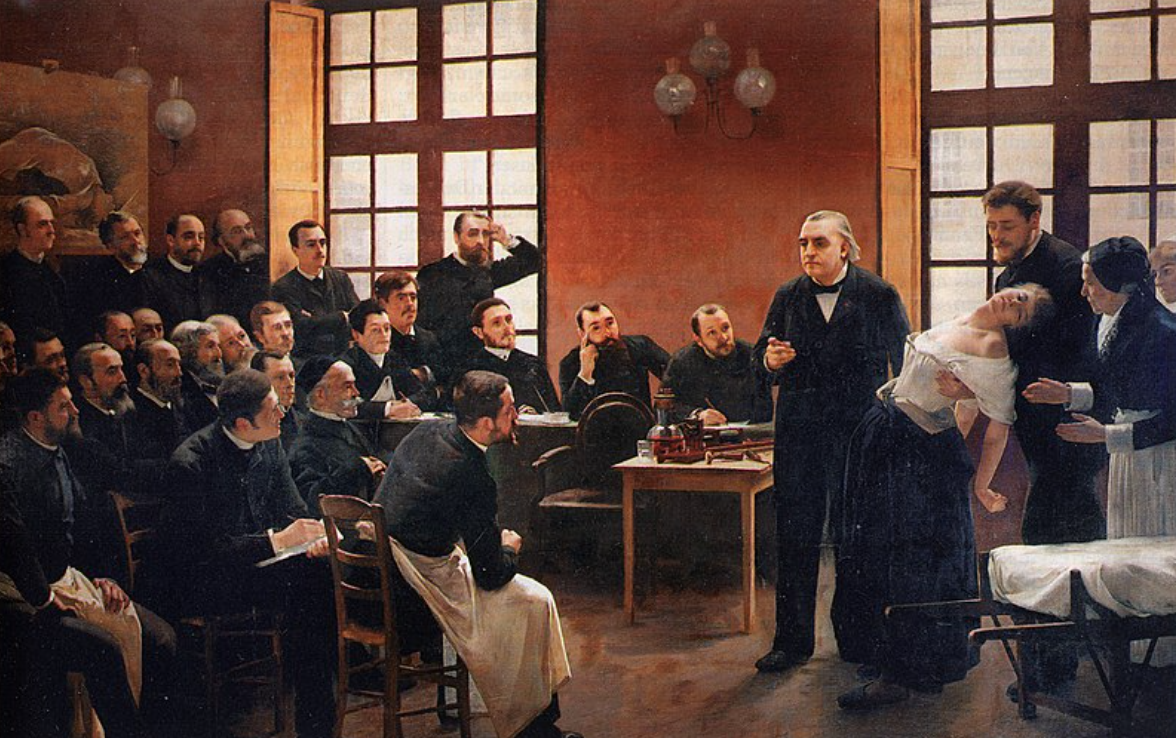
A Clinical Lesson at the Salpêtrière. The painting, one of the best-known in the history of medicine, shows the neurologist Jean-Martin Charcot giving a clinical demonstration with patient Marie Wittman to a group of postgraduate students.
From the writings of Masson and Szasz we can deduce that since those times, not only has there been a conspiracy between psychiatrists and controlling family members, but also another conspiracy between psychiatrists and the State. For example, when, after escaping and publishing her book, Hersilie appealed to the French Ministry of Justice, it sided with the psychiatrists: ‘But our doctor, who knows more about this than we do, is convinced that she is insane, and we bow to his infallible science’.[13] Hersilie’s was not the only 19th-century case unearthed by Masson, but the pattern of events is similar: young, perfectly sane women diagnosed with ‘moral insanity’ despite the doctors’ acknowledgment that there was nothing wrong with their intellect (which is why they called it folie lucide). This ‘infallible science’, according to the French Ministry of Justice’s pronouncement, hospitalized many sane people.
A parenthesis. I’m not using these examples to promote feminism or criticize the practice of black slavery in North America. I believe in patriarchy, but not in a patriarchy based on a pseudoscience that claims that liberated women of the 19th century suffered from an illness that should be treated by doctors (something analogous to today’s pseudoscientific claim that children who are distracted in school have an illness that should be treated with drugs). I could say something similar about black fugitives. They should have been deported to Africa; doctors shouldn’t have invented fake diseases.
Another curious psychiatric label for upper-class single women who had suitors from lower social strata—and here I can’t help but think of the plot of the movie Titanic—was nymphomania.[14] There were cases in which these women were committed in their prime, only to be released as old women to a nursing home. Below I quote part of a letter from Dr Massini to Dr Binswanger to commit Julie La Roche to a Swiss asylum:
In mid-January she ran off from there, supposedly with her brother, but in fact with the adventurer von Smirnoff, and suddenly appeared in Basel, presenting him as her fiancé. Here of course the relationship was not approved…
All of this leads me to conclude that Miss La Roche, who is otherwise a thoroughly lovable girl, is heading toward ‘moral insanity’, which makes medical supervision advisable… She will surely attempt to escape, perhaps at least pretend to commit suicide. It will therefore be necessary to put her in charge of incorruptible guards who will watch over her very closely… I do not believe that Mr. La Roche ever mistreated his daughter, though he may well have reprimanded her harshly.[15]
One might think that these are relics of a bygone medical past, having nothing to do with our civilized times. But this last line from Massini reminds me of Amara: to declare with all his authority my parents’ innocence in the face of my accusations and, furthermore, to have suggested I should be committed—just what Massini did with Julie La Roche. This woman’s accusation had been the following:
My father abused me in a terrible manner… after he had thrown a sharp object at my head with such force that my face was covered with blood, to which a deep wound testified. There are witnesses to all these events.
One day in Saarburg, where we returned after our marriage [with von Smirnoff], and where I had to remain in bed, we were surprised by the police and then by my father. Though sick, I was dragged off through storm and rain by Mr. La Roche [her father]. My marriage certificate, everything was in vain. With court transportation, I was taken to Kreuzlingen, which is a private insane asylum (as can be ascertained by looking it up in any directory). There, on the first day, I was diagnosed as melancholic and insane.[16]
Like Hersilie, Julie managed to escape and left us her testimony, originally published in the Swiss newspaper Thurgauer Tagblatt. And also, as in the case of Hersilie, the doctors united to confront the accusation. Julie was never vindicated by society. The newspaper where her accusation appeared had to publish a shameful retraction asserting that Julie did, indeed, suffer from moral insanity.[17]
Masson comments that if any insanity existed, it came from the father and the psychiatrists, not from the girl. Public opinion among Swiss citizens, or French in Hersilie’s case, deferred to the family institution represented by the father as well as the medical establishment and the State.
19th-century labels were not always invented to stigmatize second-class citizens like women: sometimes they were invented to avoid stigma among the privileged classes. When a daughter from a good family stole and was arrested, a psychiatrist was asked to diagnose her as suffering from kleptomania: an illness whose symptom was an uncontrollable compulsion to steal.[18] Thus, the law was circumvented and the daughter was able to return home. But just like stigmatizing labels, it is evident how the authorities openly colluded with psychiatrists to avoid, or provoke, social sanctions.
These diagnoses—‘drapetomania’ and ‘dysthesia ethiopica’ for blacks, ‘moral insanity’ and ‘nymphomania’ for women—may seem laughable to us. Values have changed so much that the essentially political nature of labels and the role of psychiatrists as agents of the system are clearly visible.
However, although with more obscure, technical, and difficult-to-detect labels, the situation today remains essentially the same. Labelling a child ‘hyperactive’ or an adolescent ‘schizoid’ only mystifies realities that can be expressed in the vernacular: naughty child, withdrawn teen. Furthermore, as in the case of societies where blacks and women were discriminated, these pseudo-diagnoses obscure the political actions that are desired to be taken. I say pseudodiagnoses because no doctor has ever been able to see under a microscope the deteriorated nervous tissue of a hyperactive child or a teenager labelled as schizoid. The new illnesses are as chimerical as the old ones: they exist only in the minds of ideologues whom people call psychiatrists but who are actually advocates for parents who wish to take control measures with their offspring.
Leaving aside genuinely pathological cases, it can be said that in past centuries and today, the hidden objective of psychiatry is control, especially of rebellious members of society: black fugitives and liberated women of yesteryear, or the young population today. That this policy persisted in the 20th century is confirmed by the statements of Francis Braceland, president of the American Psychiatric Association during the hippie movement of the 1960s. Braceland declared:
It is a feature of some illnesses that people do not have insight into the fact that they are sick. In short, sometimes it is necessary to protect them for a while from themselves… If a man brings his daughter to me from California because she is in manifest danger of falling into vice or in some way disgracing herself, he doesn’t expect me to let her loose in my hometown for that same thing to happen.[19]
It couldn’t be clearer. Note how psychiatrists haven’t changed since the 17th century, when they sent these daughters ‘in evident danger of being debauched’ to the Salpêtrière Hospital in Paris. Needless to say, the behaviour of these adolescents, both in the 17th and 20th centuries, was rebellion, not a mental disorder. Activists like Phyllis Chesler have written books of feminist philosophy on the subject, such as Women and Madness. Once again, I believe in patriarchy and I’m not against disciplining a spoiled teenager. But there’s a great danger in inventing pseudoscientific conditions that the medical profession must treat against the will of the ‘patient’ as if these behaviours were ‘diseases’.
Let us now look at psychiatry in even more recent times. In the brochure Schizophrenia, published in 1998 by the Royal College of Psychiatrists of England and the National Council on Schizophrenia of that country, we can read: ‘How do families react if a son or a daughter, a brother or a sister develops schizophrenia and becomes odd and unpredictable? They may regard the change in behaviour as rebellious, perverse and unacceptable without at first realising that it is due to mental illness’.[20]
The brochure doesn’t ask how the parents appear to the teenager. It doesn’t ask, for example, ‘Is your mother so intrusive that she treats you like a child? Is she tyrannical, possessive, and constantly bullying you, and that’s why when you distance yourself from her, you seem strange and unpredictable?’ Psychiatrists wouldn’t write a pamphlet for young people who couldn’t afford to pay them. Those who wrote the pamphlet, the official psychiatric associations in England, had ears exclusively for the parents. It doesn’t even occur to them that the young man’s version of events exists or that his rebellion could be justified. The pamphlet’s equation: rebel / perverse / unacceptable = schizophrenic reminds me that during Brezhnev’s government, the rebellion of political dissidents, a perversity unacceptable to the Russian authorities, was officially considered schizophrenia. There were many such cases, and they are well documented, but I’ll refer to just one.
In 1968, the year of the student revolts and shortly after the Soviet invasion of Czechoslovakia, Natalia Gorbanevskaya protested against the invasion in Moscow’s Red Square. She was arrested in August of that year and sent to a psychiatric hospital called the Serbsky Institute. The chairman of the commission, Professor Morozov, diagnosed Natalia as suffering from ‘a chronic mental illness, type of schizophrenia’. The commission concluded that Natalia showed changes in her reasoning process and in her critical and emotional faculties. It was concluded that Natalia had participated in the Red Square demonstration in a state of mental illness and was hospitalized.[21] Even before Brezhnev, Nikita Khrushchev had stated in Pravda: ‘Crime implies a deviation from generally approved standards of conduct, and its cause is often mental disorder… It is evident that the mental state of those who call for opposition to communism is not normal’.[22]
Rebellious women have fared no better in the West. As Chesler wrote a few decades ago, statistics continued to show that women were labelled psychiatrically more frequently than men; they were given far more antidepressants and sometimes continued to be hospitalized by their husbands or relatives. I myself heard of a wealthy Opus Dei family in Monterrey, Mexico that at the beginning of the new century used psychiatry to hospitalize a daughter when she divorced—an inconceivable sin for those in Opus Dei—to run off with a rocker. According to what Alejandro Fonseca, the rocker, told me personally when I interviewed him in Monterrey in August 2004, his partner remained imprisoned by her family. The fact that the West has criticized what Soviet psychiatry did to Natalia while similar measures are taken with women in our hemisphere is a double standard.
But returning to the English pamphlet. Its target readership was the general population of the United Kingdom. According to American and European psychiatric manuals, the five symptoms of schizophrenia are: (1) hallucinations, (2) delusions, (3) disorganized thinking, (4) extremely disorganized behaviour, and (5) catatonic behaviour: two of the five symptoms are required for a diagnosis of schizophrenia. However, the UK pamphlet reads something similar to what the Serbsky Institute commission did to Natalia: that the family of the (pseudo) schizophrenic ‘may see the change in behaviour as rebellious’ without understanding ‘that it is due to an illness’. In other words: in practice, and quite independently of disturbed behaviour, adolescent rebellion can be an illness: schizophrenia. Women’s liberation in the 19th century could be seen as an illness: moral insanity. The black slave’s desire to escape was an illness: drapetomania. All of these ‘illnesses’ have required medical intervention, which frequently ends in imprisonment without legal trial. In this regard, in another part of the same pamphlet we read: ‘People with schizophrenia do not always realise they are ill and may refuse treatment when they badly need it. In these circumstances, the Mental Health Act in England and Wales [enacted in 1983] and similar legal arrangements in other countries, permit compulsory admission to hospital’. [23]
Please note that this is a pamphlet published in 1998, and that I obtained it during a sort of social service during my Open University course of 1999. As I said above, psychiatric positions have not changed since the days of American slavery or European sexism; only social values have. Psychiatrists have always behaved, and continue to behave, as agents of the current status quo: whether they are landowners in the American South, fathers who abhor their daughters’ plebeian affairs, or controlling mothers who tolerate no independence in their children.
Another kind of evidence of the alliance between parents and psychiatrists comes from someone who left the profession of psychoanalysis and whom I have quoted in previous pages: Jeffrey Masson. In Final Analysis, one of the books I most treasure because it opened my eyes to understand what Amara did to me, Masson tells us:
“When a child manifests gross pathology…” These words startled me into consciousness. They were enunciated, for emphasis, very slowly, and in a booming voice. There could be no doubt about it, the department chairman was a fine orator. He had acted on the stage. His voice, his urban wit, his friendliness, his poise and his great knowledge of literature were all admirable. He laughed a great deal. He liked to make jokes. You had to like him.
But you did not have to like what he said. And I did not. What was it to “manifest gross pathology”? In this case, an eight-year-old boy was the “identified” patient. The word “identified” was a popular and venerable psychiatric term. He had been “identified” as the patient by his mother and father, simply because he was not doing well at school, he had few friends, and he was a “problem” at home. How was this, I wondered at the time, “gross pathology”? Where was I? I was at grand rounds. [24]
The grand rounds were the visits to a psychiatric hospital in Toronto during Masson’s psychoanalytic training. Masson is the only analyst in the world who has dared to expose, in several books, ‘the indoctrination process’ of this ‘semi-secret society’ that is the training of psychoanalysts. During the meetings, the hospital staff would gather and a senior psychiatrist would present the case of one of the hospitalized patients which, Masson observed, was humiliating for the latter. ‘It soon became apparent that every presentation of therapy was only good as the intellect and heart of the presenter. You did not, you could not, learn about the patient, but you learned plenty about the presenter… So here was a department chairman talking about still another “patient”, Jill, nineteen, “who was admitted to the hospital with a schizophrenic psychotic decompensation”.’ [25]
The director of the department that presented these cases was a respected psychiatrist who believed in the appropriateness of electroshock therapy. Masson continues:
How did we know, for example, that somebody was “sick”? It was simple: they were brought to the hospital. The chairman made it clear that a person who had been “identified” as a patient by the family, was, in fact, disturbed in a psychiatric way. People apparently did not err when it came to making these kinds of home diagnoses. Thus, he told us, speaking of the “maladjusted” (a medical term?) child, that we should accept “that the ‘identified’ patient is ‘sicker’ than the others. A study by S. Wolff (in the British Journal of Psychiatry) lends support to the family’s identification of its most disturbed member as the ‘sick one’…” To me, this was suspiciously convenient for the psychiatrist. What gave the psychiatric community this power? [26]
Who gives them special powers over children and adolescents? Society and its laws, of course; the State, the culture itself!
In 1995, a study published by American psychiatrists concluded that family members are just as capable as professionals of ‘identifying’ behaviour that requires involuntary hospitalization.[27] Another piece of evidence of a conspiracy between parents and psychiatrists is suggested by the fact that the official psychiatric organization in the US, the American Psychiatric Association, has entered into open collaboration with one of the most despicable organizations in North America: NAMI. Many members of the National Alliance for the Mentally Ill are parents who wish to take repressive measures against their children. Their stance has been so extreme that it has gone so far as to justify lobotomy and harass psychiatrists who do not practice the bio-reductionist faith.[28]
It is important to be aware that this alliance between tyrannical parents and psychiatrists is a very old story, and one that continues unchallenged in our societies. In my own case, when I complained to my father in 1991 that he and my mother had ignored the accusations in my Letter to mom Medusa, that they had ‘ignored it, took no action on it’, he responded in writing: ‘We didn’t shelve anything down; we paid your psychiatrist and saw others. Everyone, including Amara, accepted that we were right’ (emphasis in the original by underlining).
Why are psychiatrists able to ‘accept’ that the parents who have horrendously abused a child ‘are right’? Why do they always blame the child and exonerate the adult? In the Letter I delved into my parents’ minds but not into what might have gone on in the mind of the doctor who acted as their representative. Now, twelve years after writing it, I think I’m ready to analyse analysts, even if that task will take me the rest of this book.
____________
[1] Videotaped speech by Thomas Szasz at the headquarters of the Citizens Commission on Human Rights in Los Angeles, California (February 28, 2004).
[2] Quoted in Thomas Szasz: The Manufacture of Madness: A Comparative Study of the Inquisition and the Mental Health Movement (Syracuse University Press, 1997), p. 14.
[3] Ibid., pp. 48f.
[4] Ibid., p. 308.
[5] Quoted in Thomas Szasz: Pharmacracy: Medicine and Politics in America (Praeger, 2001), p. 90.
[6] Robert Mendelssohn, quoted in Breggin: Toxic Psychiatry, p. 298.
[7] Joe Sharkey: Bedlam: Greed, Profiteering, and Fraud in a Mental System Gone Crazy (St. Martin’s Press), 1994, pp. 12 & 98.
[8] Paul Fink, quoted in Breggin: Toxic Psychiatry, p. 360. I read about these million-dollar earnings in Sharkey: Bedlam, p. 202.
[9] Daniel Defoe, quoted in Thomas Szasz: Esquizofrenia (México: Ediciones Coyoacán, 2002), p. 133. The text in which Defoe spoke out against the psychiatry of his time is titled “Demand for Public Control of Madhouses”.
[10] Quoted in Sharkey: Bedlam, p. 182.
[11] Whitaker summarizes Benjamin Rush’s psychiatric work in the first two chapters of Mad in America.
[12] Quoted in Jeffrey Masson: Against Therapy (HarperCollins), 1999, p. 57. The alliance between parents and psychiatrists is particularly discussed in chapters 1, 5, and 6.
[13] Ibid., p. 22.
[14] Roger Gomm: “Reversing Deviance” in Tom Heller (ed.): Mental Health Matters (The Open University, 1996), p. 80.
[15] Masson, Against Therapy: pp. 70f.
[16] Ibid., 72f.
[17] Ibid., p. 76.
[18] Gomm: Mental health matters, p. 80.
[19] Quoted in Szasz: The Manufacture of Madness, pp. 46f.
[20] Schizophrenia (National Schizophrenia Fellowship & Royal College of Psychiatrists, 1998), p. 12.
[21] Víctor Miguel Lozano: “la psiquiatría y la psicocirugía como instrumentos de represión” in Alternativas, pp. 207 ff.
[22] Cited in Paul Johnson: Tiempos Modernos (Ediciones B, 2000), p. 834.
[23] Schizophrenia (pamphlet, op. cit.), p. 9.
[24] Jeffrey Masson, Final Analysis: The Making and Unmaking of a Psychoanalyst (Harper Collins, 1991), pp. 48f.
[25] Ibid., pp. 50f.
[26] Ibid., p. 51.
[27] J. R. Husted and A. Nehemkis: “Civil Commitment Viewed from Three Perspectives: Professional, Family, and Police” in Bulletin of the American Academy of Psychiatry Law (1995; 23, 4), pp. 533–546.
[28] Breggin: Toxic Psychiatry, pp. 425f. NAMI also tried to boycott Loren Mosher’s humanitarian project: a kind-hearted psychiatrist with his inpatients.
2 replies on “Sample chapter”
HOJAS SUSURRANTES
(Whispering leaves):
Letter to mom Medusa
How to murder your child’s soul [the 2nd chapter / “book”]
My childhood
The return of Quetzalcoatl
Whispering leaves
______ 卐 ______
TABLE OF CONTENTS TO CHAPTER (“BOOK”) II
Foreword
Dad and Mum:
Introduction
Psychiatric re-victimisation and demolishing panic of the inner self
Abusive parents and psychiatrists: A felonious association [the text translated above]
The nature of evil: Amara (I)
States within the state: laws and psychiatry
Inside the Ministry of Love
Shine: a dad more devastating than Mengele
The nature of evil: Amara (II)
The nature of evil: Amara (III)
‘I never did anything ignoble’ —Freud
The nature of evil: Amara (IV)
How to murder your child’s soul
Appendix I:
From the Great enclosure to chemical Gulag
Appendix II:
Why psychiatry is a false science
A most critical evaluation; I have enjoyed every word, and have so much new to learn too. I like the entire gist. Sounds harsh, but necessary…